


The potential of PARP inhibitors in prostate cancer: What nurses need to know (Episode 2 of 3 – English)
The potential of PARP inhibitors in prostate cancer: What nurses need to know (Episode 2 of 3 – English)
In the second episode of this podcast series, Pablo Peinado and Dr Elena Castro discuss PARP inhibitors, how they work, review key trial data, how to select PARPi’s for their prostate cancer patients and where they fit in the overall treatment sequence.
In the second episode of this podcast series, Pablo Peinado and Dr Elena Castro discuss PARP inhibitors, how they work, review key trial data, how to select PARPi’s for their prostate cancer patients and where they fit in the overall treatment sequence.
Dr. Elena Castro, Pablo Peinado
Listen to Episode 2 - The potential of PARP inhibitors in prostate cancer: What nurses need to know

Dr. Elena Castro
Medical Oncologist
Hospital Universitario Virgen de la Victoria
Spain

Pablo Peinado
Research Nurse
Hospital Universitario Virgen de la Victoria
Spain
![]() Podcast |
Podcast | ![]() 25 min
|accreditation:
EACCME |
Jan 2022
25 min
|accreditation:
EACCME |
Jan 2022
download resources

This programme was made for you: your opinion matters
Share your feedback in just 4 clicks and help us to continue to create the content you need.
I agree that this educational programme:
Podcast Episode 2: The potential of PARP inhibitors in prostate cancer: What nurses need to know
Brought to you by:
Pablo Peinado, Hospital Universitario Virgen De La Victoria, Málaga, Spain
Dr Elena Castro, Hospital Universitario Virgen De La Victoria, Málaga, Spain
Please note: GU NURSES CONNECT podcasts are designed to be heard. If you are able, we encourage you to listen to the audio, which includes emotion and emphasis that is not so easily understood from the words on the page. Transcripts are edited for readability. Please check the corresponding audio before quoting in print.
This GU NURSES CONNECT programme is supported through an independent educational grant from AstraZeneca. GU NURSES CONNECT is an initiative of COR2ED.
The views expressed within this podcast are the personal opinions of the authors. They do not necessarily represent the views of the author’s academic institution, or the rest of the GU NURSES CONNECT group.
Pablo Peinado: Hello, and welcome to the second podcast in the series covering PARP inhibitors in prostate cancer. Today we are going to be discussing the potential of PARP inhibitors in prostate cancer: What nurses need to know.
I am Pablo Peinado, and I am a research nurse coordinator at the GU unit in Virgen De La Victoria Hospital, Málaga, south of Spain and I'm a member of the GU Nurses CONNECT. I am delighted to be joined today by my colleague, Dr Elena Castro, who is a medical oncologist also working at the Hospital Universitario Virgen De La Victoria Hospital in Málaga Spain as well, thanks for joining me today, Elena.
Elena Castro: Thank you Pablo, it's my pleasure.
Pablo Peinado: So, Elena we've been both working with PARP inhibitors for some time, initially through involvement in clinical trials. Perhaps you could provide us a brief overview of PARP inhibitors and how they work?
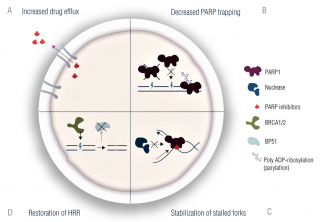
Elena Castro: What PARP inhibitors do is to inhibit the function of PARP.
PARP is a family of proteins, the most frequent ones are PARP1 and PARP2, that are involved in repairing the damaged DNA. The cells have different mechanisms to repair DNA damage and when these inhibitors prevent PARP from doing its work in most cells there will be other mechanisms that can overcome the functions of PARP. But in those cells that have damage in other DNA repair mechanisms, as is the case of cells with alterations in BRCA 1 or 2 the cell will not be able to repair the damage and will accumulate a number of alterations and the cell finally will die.
So, it is important that in prostate cancer about 20% of tumour's have alterations in these pathways, particularly in the homologous recombination pathway. The tumours that have alterations in the homologous recombination pathway are the tumours that are more sensitive to treatment with these PARP inhibitors.
Pablo Peinado: Thank you, Elena that was really interesting. Over the past couple of years, we've seen two PARP inhibitors receive regulatory approval which are olaparib and rucaparib.
What can you tell us about the trials for these two treatments, TRITON2 and PROfound which led to these approvals?
Elena Castro: Yes, as you mentioned for rucaparib is the TRITON2 trial, it's a phase 2 trial that has already been reported. For olaparib we already know the data from phase 2 trials, but also from the phase 3 trial, PROfound.
So, I will start with TRITON2 that is a phase 2 trial of rucaparib in patients with metastatic castration resistant prostate cancer, whose disease has already progressed to treatment with an androgen receptor targeting inhibitor such as abiraterone or enzalutamide and also to taxane based chemotherapy.
So, these patients were screened for alterations in BRCA1/BRCA2 and in other genes involved in DNA damage repair which are frequently named DDR genes. And patients who have these alterations and have previously received the therapies I mentioned, were allowed in the trial and they received treatment with rucaparib, 600 milligrams twice a day.
So, the primary endpoint of the study was objective response rate, so radiographic response rate, and the secondary endpoints were duration of these radiographical response, the PSA response rate, the time to PSA progression and radiographic progression-free survival and overall survival.
So, what was observed in this trial was that for patients with alterations in BRCA1 and BRCA2 about 40% of them achieved radiographic response, and 50% of them achieved PSA response and I think this is very relevant because we must remember that these patients have already received at least two lines of therapy for their disease. So, I think this is very remarkable.
For patients with alterations in other DDR genes such as ATM or CHEK2, the radiographic response rates and PSA response rate were significantly lower, around 10%. So, this suggests that the patients with alterations in BRCA1 and BRCA2 are the ones that benefit the most from PARP inhibitors.
Pablo Peinado: Thanks Elena for a great overview of the TRITON2 study, perhaps you could tell us now something about the PROfound study, how the two studies differ?
Elena Castro: The PROfound study has been the first randomised phase 3, biomarker driven trial in prostate cancer. I know we have several other biomarker driven trials in other diseases, but in prostate cancer, this has been the first one.
So, patients, with alterations in at least one of the 15 genes involved in homologous recombination that were tested in this study. If they were positive, they have one of these alterations, patients were eligible for the trial.
And patients were divided into two groups. In cohort A were included those patients with alterations in BRCA1, BRCA2 or ATM because these patients were the ones that were expected to respond better to olaparib. And cohort B included patients with alterations in the other 12 genes that were tested.
So, all patients to be included in the study have previously received treatment with an androgen receptor targeting therapy, abiraterone, enzalutamide. And taxane treatment was not mandatory, previous treatment with taxane-based chemotherapy was not mandatory, but it's still about 70% of patients in the trial had already received chemotherapy as well.
So, patients within each cohort, cohort A and cohort B, were randomised to receive either olaparib, 300 milligrams twice a day, or a second hormonal therapy, usually the one that they have not received before.
And the primary endpoint of the PROfound study was radiographic progression-free survival in cohort A. I mean in patients with alterations in BRCA1, BRCA2 and ATM.
And the secondary endpoints included radiographic progression free survival in both cohorts together, A and B, and overall survival in cohort A.
So, the most important results that have been reported, is that the medium overall survival in cohort A for patients who received olaparib was 19 versus 15 months for those patients who receive a second hormone therapy. So, the difference was statistically significant, and the risk of death was reduced by 30% in those patients treated with olaparib.
So, cross over from the control arm to olaparib was allowed at the time of radiographic progression and in a sensitivity analysis that took into consideration this cross-over, olaparib showed 60% decrease in the death risk in those patients with alterations in BRCA1, BRCA2 and ATM altogether.
So, this has been the first phase 3 trial with a PARP inhibitor in prostate cancer reported so far, and this led to the approval of olaparib to treat these patients.
Pablo Peinado: Okay, so thank you Elena for this information about the two studies, TRITON2 and PROfound study. Now we would like to know a bit more about what the safety profiles from these trials are.
Elena Castro: The safety was very similar in both trials and similar toxicities were observed. The most frequent side effect with PARP inhibitors is asthenia, fatigue and also anaemia. So other frequent side effects are nausea, a decreased appetite, thrombocytopenia, so most of the patients in the trials experienced some toxicity, but in most cases, it was grade one or two and did not require treatment discontinuation.
So, anaemia and thrombocytopenia were the main causes of treatment interruption. About 40% of patients require a dose reduction, at some point, mostly because of anaemia. So, anaemia was easily managed with treatment temporary interruption, supported therapy and then the treatment was re-introduced with a dose reduction. So overall the treatments are quite well tolerated.
Pablo Peinado: So, Elena based on you on the data that you've just shared with us how do you select which PARP inhibitor, to give to the patient and where do PARP inhibitors fit into the treatment sequence for advanced prostate cancer patients?
Elena Castro: At present we don't have data to select one PARP inhibitor over another, based on efficacy or toxicity, and in most cases, we will select one over another based on availability. So, it is interesting how the regulators have interpreted the data differently in the European Union and the States for instance. So rucaparib at present is not approved in Europe, yet. It is approved in the States for patients with alterations in BRCA1 or BRCA2 only who have already received treatment with an androgen receptor targeting therapy and taxanes.
Olaparib has been approved in both the States and Europe. In Europe, the regulators have understood that the patients that benefit the most are those with alterations in BRCA1 or BRCA2 and at present it's only approved for patients with alterations in those genes who have already received treatment with androgen receptor targeting inhibitor. In the States the regulators have approved olaparib for patients with alterations in 14 homologous recombination repair genes, provided that the patient had already received treatment with a hormone agent.
So, we've talked about the trials for the two approved PARP inhibitors and Pablo as you were involved in these trials, I would love to hear what were the main questions or concerns that you have from the patients?
Pablo Peinado: Well Elena, first of all, we should consider that those patients have already received a couple of lines of treatment which makes them really aware about the disease, the therapies for the current situation. The difference now is that they've been diagnosed with DNA repair alteration, and this opens a new stage in their disease. This new diagnosis implies the possibility of receiving a PARP inhibitor, which is the best treatment for them, and they are really looking forward to it.
But on another hand once the discussion about the implications of these diagnoses continues, the patient usually expresses their concerns about the consequences for their relatives. Will they have the same alteration? Will it affect their health? Can they pass it onto the children? Those are really important questions that we should be ready to answer. At the same time that we can refer them to the genetic counselling clinic where they can give them a lot more information on that.
Their prognosis is one of the most important concerns that they have. They know their prognosis is not good, and they want to start the treatment as soon as possible. So, we should really encourage them to focus on the process and go, step by step in their treatment trying to make sure they understand everything while we go along.
Elena Castro: Thank you Pablo, I think it's very, very interesting what you just said. What do you think are the main points for the nurse to communicate to their prostate cancer patients regarding treatment with PARP inhibitors?
Pablo Peinado: Well, as we see in our daily clinic the patients usually have a closer relationship with us as nurses than they do with the doctors. That happens because we spend a lot of time speaking with them, while we perform other procedures such as blood tests, give them appointments etc. and this allows us to build a closer relationship with them, and we should use this confidence to help them during this new stage of their disease.
However, advanced prostate cancer patients are usually more than 60 or 70 years old. Some of them not highly educated, so we can imagine how difficult it is for them to understand a DNA repair alteration diagnosis. We have to use a simple vocabulary, all the time checking at every step that they have understood everything because, probably, they will have to explain it again to their relatives once they go home. So, it is really important to use an inclusive vocabulary and allow them to ask any question about it during the process.
As we've seen in the data that you just presented for both studies, there is a considerable risk of suffering an adverse event such as anaemia, fatigue, nausea. So, we can identify some of these adverse events with a blood test or some other procedures but there are others, such as fatigue, nausea or lack of appetite that are not so easy to diagnose. The communication with our patient is crucial. We have to make sure they are able to identify those adverse events as soon as possible, so they can inform us and we can treat them to prevent them getting worse.
At the end we should accomplish some objective with this patient. We have to make sure that our patient leaves the clinic with a clear vision of their new DNA repair alteration diagnosis.
At the same time, they should understand the treatment, how they have to take their medication and how does it work. And we have to make sure they are able to identify the possible adverse events, so we can prevent that happening.
We've talked in depth about the key trials but now we focussed our discussion so far on the two approved PARP inhibitors but are there other PARP inhibitors in development that we should be aware of?
Elena Castro:
Yes, other PARP inhibitors that have proven to be effective in other tumour types are also being tested in prostate cancer.
That is the case of niraparib and talazoparib. Phase 2 trials with these drugs have already been reported that is GALAHAD for niraparib and TALAPRO-1 for talazoparib. And in these two trials patients with similar characteristics to those included in the TRITON2 trial, that we just discussed, were enrolled. And what has been observed is that the radiographic response rates in all these phase 2 trials were very similar with the different agents. So, the patients that benefit the most are those with alterations in BRCA1 and BRCA2 and the objective response rates have been over 40% with the different PARP inhibitors with similar PSA responses, around 50%.
So, what we've learned from all these trials with PARP inhibitors in prostate cancer is that the patients that benefit the most from these therapies are those with alterations in BRCA1 and BRCA2 even when they may be heavily pre-treated. But we have another group of frequent alterations, such as those in ATM and CDK12 that don't seem to sensitize patients to respond to PARP inhibitors or at least not in monotherapy.
And finally, we have some other alterations that are less frequent, and, in consequence, the number of patients included in the trials is small. To get strong evidence for the benefit of PARP inhibitors in these patients we may have to wait to pull together the results of different trials and results from real word studies in order to get enough number of patients with this rare alterations to understand whether these patients benefit or not from these therapies.
Pablo Peinado: So then, there are a number of ongoing trials looking at PARP inhibitors in prostate cancer in combination with other treatments, perhaps you could comment on how you think this combination may benefit patients?
Elena Castro: Yes, what is being done is to combine PARP inhibitors with androgen receptor targeting inhibitors, for instance enzalutamide or abiraterone, because there is a cross-talk between the androgen receptor and the DNA repair mechanism.
So, what is being tested is whether the combination of these two drugs could result in a benefit for patients without DNA repair defects, meaning that a larger number of patients could benefit from these combinations compared to those that benefit from PARP inhibitors in monotherapy.
So, these drugs are also being tested in combination with immunotherapy, in combination with radium 223, in combination with lutetium, so just trying to benefit a larger number of patients by taking advantage of potential synergies. But we need to wait to get the results of all these trials.
It's also important that some of these PARP inhibitors may not seek approval in monotherapy, but the companies may try to get them approved in combination with other therapies already available for patients with advanced prostate cancer.
Pablo Peinado: Well, thank you, Elena for this great discussion. What are your take home messages for our listeners then?
Elena Castro: Well, I think we have a new class of drugs to treat our patients with advanced disease and these drugs are safe and their side effects are easily managed in the clinic and these drugs are well tolerated. These drugs work in patients with certain DDR alterations and in order to identify those patients that may benefit from these therapies, we need to test their tumours. That could be done in different ways, we can test the tumour, we may need to repeat a biopsy, we can test circulating DNA.
We need to make sure that our patients understand what we need to do, and we need to explain to them and to be aware that this is something that could be difficult to understand for them. Well, this is why we are here for and I'm sure these are exciting times for prostate cancer and precision oncology has arrived to prostate cancer with PARP inhibitors.
Pablo Peinado: Thanks again Elena, and thanks to our listeners and we encourage you to tune into the other two podcasts in this series on PARP inhibitors in prostate cancer, thank you very much.
The potential of PARP inhibitors in prostate cancer: What nurses need to know (Episode 2 of 3)
In this episode, Pablo Peinado and Dr Elena Castro discuss PARP inhibitors, how they work, review key trial data, how to select PARPi’s for their prostate cancer patients and where they fit in the overall treatment sequence, as well providing insights into communicating with patients, PARPi’s currently in late-stage development and the potential future use of PARPi’s in combination with immunotherapies or androgen receptor pathway inhibitors.
In Episode 1, Genetic testing and PARP inhibitors in prostate cancer, Joanne Chien and Dr Alexander Wyatt discuss the gene alterations in prostate cancer and why we should consider genetic testing when thinking about treatment options such as PARP inhibitors (PARPi’s). The discussion covers why genetic testing should be performed, who should undergo testing, how to test and what this means in relation to treatment with PARP inhibitors.
Dr Alexander Wyatt explains the difference between germline and somatic mutations and Joanne Chien discusses the role of the nurse during genetic counselling discussions and how this role may evolve in the future. Finally, the ongoing trials of PARP inhibitors in combination with other prostate cancer treatments are also considered and whether the outcome of these trials is likely to impact the need to perform genetic testing.
In the third and final episode, PARP inhibitors in prostate cancer: management of adverse events and the importance of communication with patients, Dr Jason Alcorn and Dr Alicia Morgans discuss adverse events associated with PARP inhibitors and the management of them, in particular thrombocytopenia, gastrointestinal effects and fatigue. Jason provides some insight into how nurses support and communicate with patients, the importance of early reporting of side effects and how to manage these. Finally, the ongoing trials of PARP inhibitors in combination with other prostate cancer treatments are also considered and what these trials may mean for patients.
Complete the e-learning and claim your CME credit here.
This GU NURSES CONNECT podcast is also available on
Castos, Spotify, Apple Podcasts, and Google Podcasts
This educational programme has been endorsed by:
![]()
GU NURSES CONNECT is an initiative of COR2ED, supported by an Independent Educational Grant from AstraZeneca, Bayer and Eisai Europe Limited.
Other programmes of interest















Other programmes developed by Dr. Elena Castro
Dr. Elena Castro
Medical Oncologist
Hospital Universitario Virgen de la Victoria
Spain



Other programmes developed by Pablo Peinado
Pablo Peinado
Research Nurse
Hospital Universitario Virgen de la Victoria
Spain

