Integrating patient preference into treatment decisions for advanced prostate cancer
Integrating patient preference into treatment decisions for advanced prostate cancer
GU CONNECT expert, Dr. Alicia Morgans provides her perspective on how to integrate patient preference into treatment decisions for advanced prostate cancer. GU CONNECT expert, Dr. Alicia Morgans provides her perspective on how to integrate patient preference into treatment decisions for advanced prostate cancer.Assoc. Prof. Alicia Morgans
Watch the video and download the slides.
Assoc. Prof. Alicia Morgans
Medical Oncologist
Dana-Farber Cancer Institute
United States (US)
![]() |
| ![]() 5 min
|
Dec 2021
5 min
|
Dec 2021
download resources


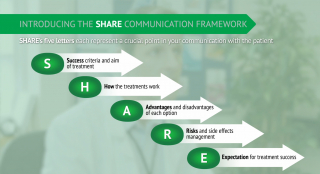
This programme was made for you: your opinion matters
Share your feedback in just 4 clicks and help us to continue to create the content you need.
I agree that this educational programme:
Hi, my name is Alicia Morgans and I'm a GU Medical Oncologist at Dana-Farber Cancer Institute.
I'm excited to talk with you today about integrating patient preferences into decision making for advanced prostate cancer.
As we know prostate cancer is really a disease spectrum and patients may enter across that spectrum and have different needs and personal preferences at different phases of their disease.
Patient-Centred Care
We as clinicians have to provide patient-centered care that considers these needs across that spectrum and really addresses what a patient is interested in or the symptoms a patient may be experiencing at that particular point in time.
Patient-centered care can improve outcomes like the patient's subjective quality of life and pain control outcomes but can also improve hard outcomes including potentially improving adherence to oral medications that patients must take to improve their cancer control.
Quality of life that patients experience is comprised of the patient-reported outcomes that patients really provide to reflect their experience in terms of pain control, physical, social or emotional functioning as well as adverse events related to the disease and its treatment.
Of course, all of this must be taken into context in the consideration of this X factor which is patient needs and patient experiences in terms of work obligations or personal obligations, personal anxieties, or preferences.
As we think about patient preferences and incorporating them into decision making, we can consider non-metastatic castration-resistant prostate cancer as an example.
Health-related quality of life
As we consider these clinical trials we can see that health-related quality of life was assessed for all of the trials that assessed treatments for this disease state and importantly all of our options improve or maintain quality of life by patient report.
We also know that the adverse events across the spectrum of the three trials that led to treatments for non-metastatic CRPC were assessed as well and were generally demonstrating good tolerability across the spectrum.
We have to consider, as I also mentioned, those X factors as we think about helping patients through decision making and so this means including conversations about obligations a patient may have personally or professionally, passed experiences that a patient may have or preferences about pain control or disease delivery modality.
Of course, as clinicians we have to work as multi-modal teams and think about how we can get the right treatment to the patient who needs it in the context of his comorbidities that we also need to ensure are managed appropriately. Drug-drug interactions are a key consideration here.
Metastatic castration-resistant prostate cancer (mCRPC) patients
As we think about particularly metastatic castration-resistant prostate cancer patients it is important to remember things that are important to them across the options for treatment that we know at this point improve disease control and hard efficacy outcomes like overall survival and progression-free survival.
In this context pain is often a key concern for patients with metastatic CRPC so providing pain control either through treatment, things like radium for example that can provide both efficacy against the cancer as well as symptom management or using external beam radiation or medications like narcotics or other pain relievers to improve pain control can be really important as we think about patients and their day-to-day quality of life.
Ultimately, we need to work together as a team, work with patients, have shared decisions and really ensure that patients have a voice that is heard in treatment decision making. We can provide the best care for patients as long as we really ensure that we include them in that process.
Please go to GU CONNECT to download these slides for more information.
Integrating patient preference into treatment decisions for advanced prostate cancer
GU CONNECT expert, Dr. Alicia Morgans provides her perspective on how to integrate patient preference into treatment decisions for advanced prostate cancer.
Watch the video and download the slides.
GU CONNECT is an initiative of COR2ED, supported by an Independent Educational Grant from AstraZeneca, Bayer and Eisai Europe Limited.
Other programmes of interest















Other programmes developed by Assoc. Prof. Alicia Morgans
Assoc. Prof. Alicia Morgans
Medical Oncologist
Dana-Farber Cancer Institute
United States (US)